Cases
ICA Bifurcation Aneurysm
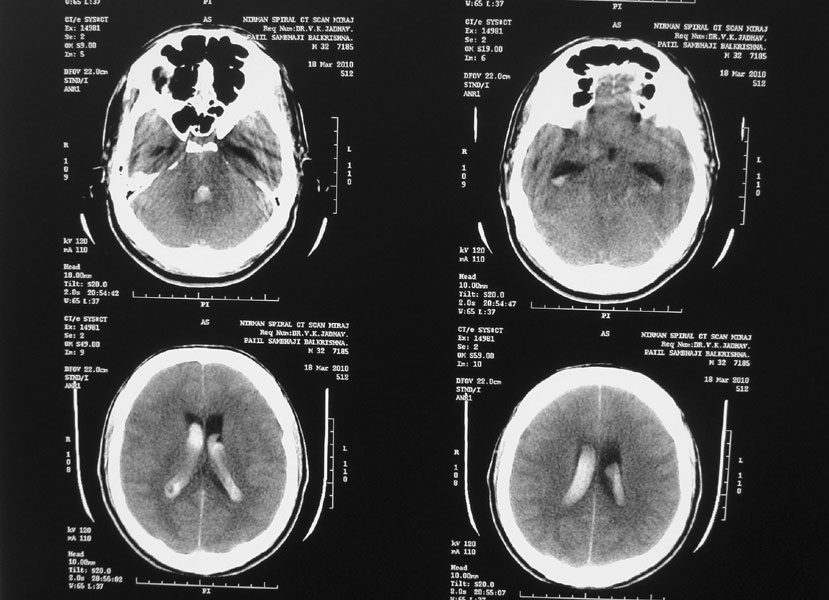
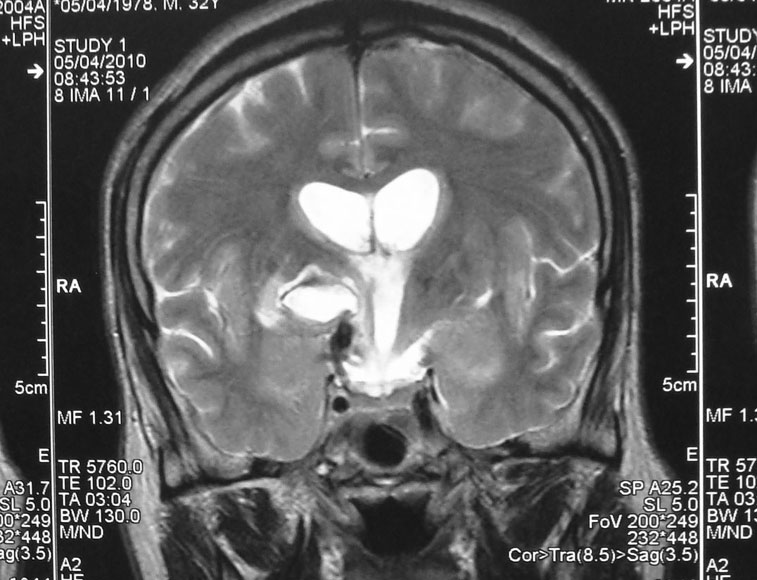
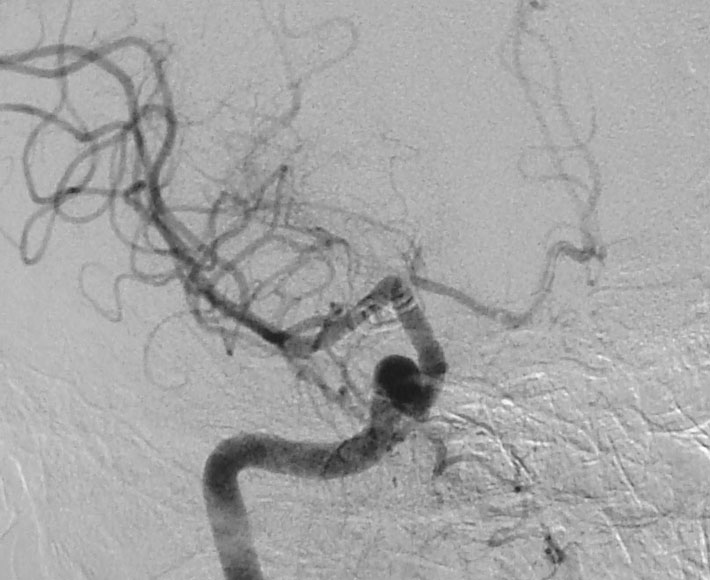
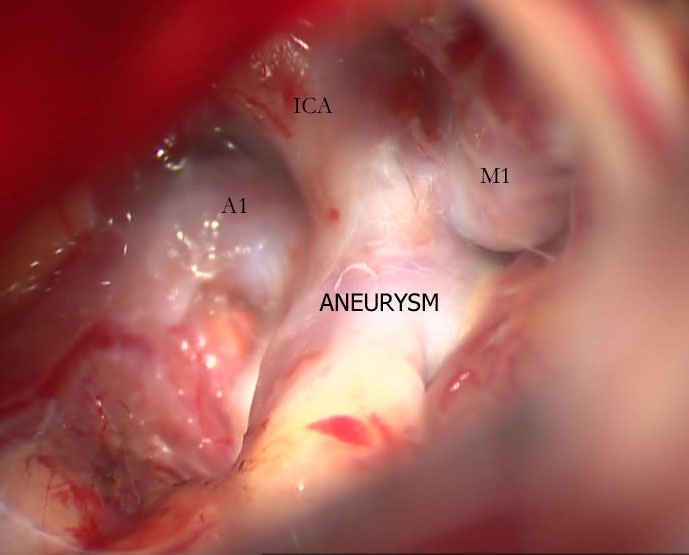
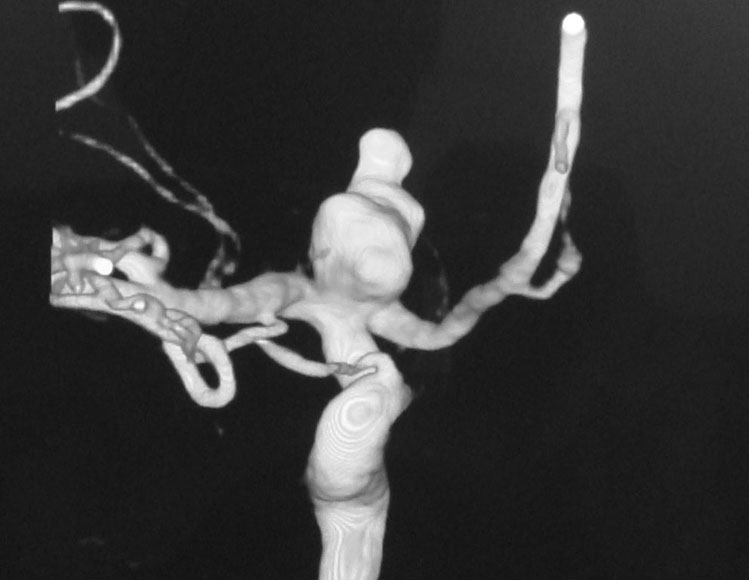
A 38-year-old-male was admitted with sudden onset of severe global headache and vomiting, followed by altereation in sensorium. CT brain showed subarachnoid and intraventricular hemorrhage (Fig 1). MRI brain revealed deep seated right sided thalamic hematoma due to ruptured internal carotid artery bifurcation aneurysm (Fig 2), confirmed by cerebral digital subtraction angiography (Fig 3). He underwent clipping of the aneurysm by transciliary supraorbital keyhole minicraniotomy (see video). Postoperative angiography showed complete occlusion of the aneurysm (Fig 4). When discharged ten days later, there was no neurological deficit (Fig 5).


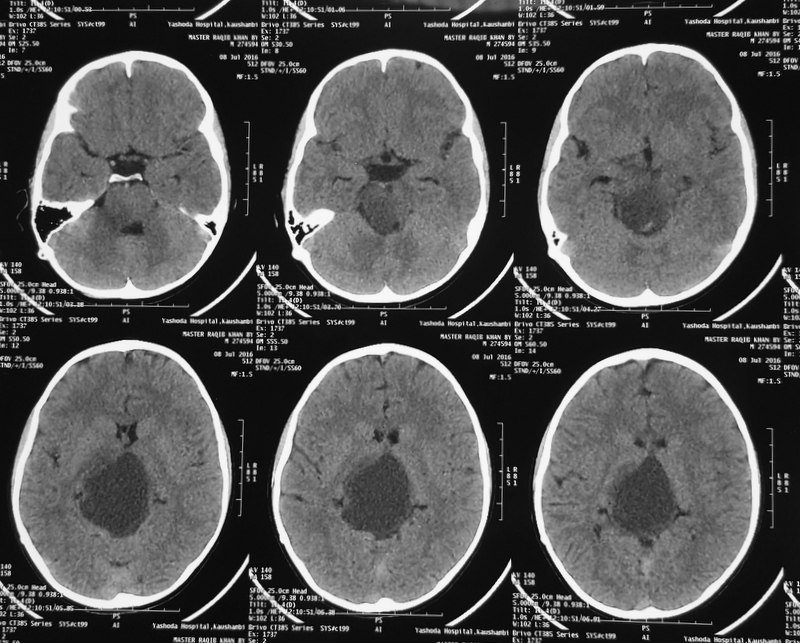
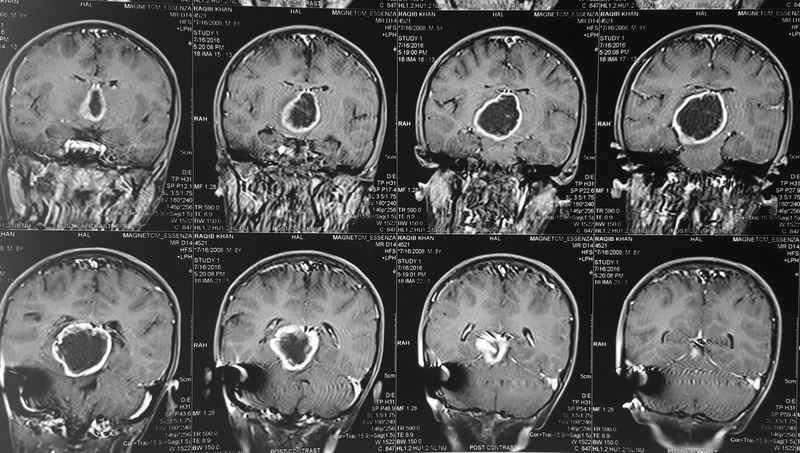
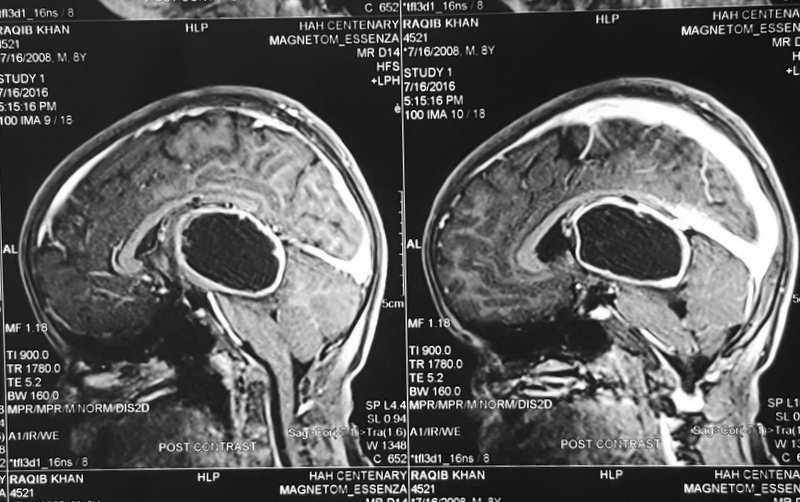
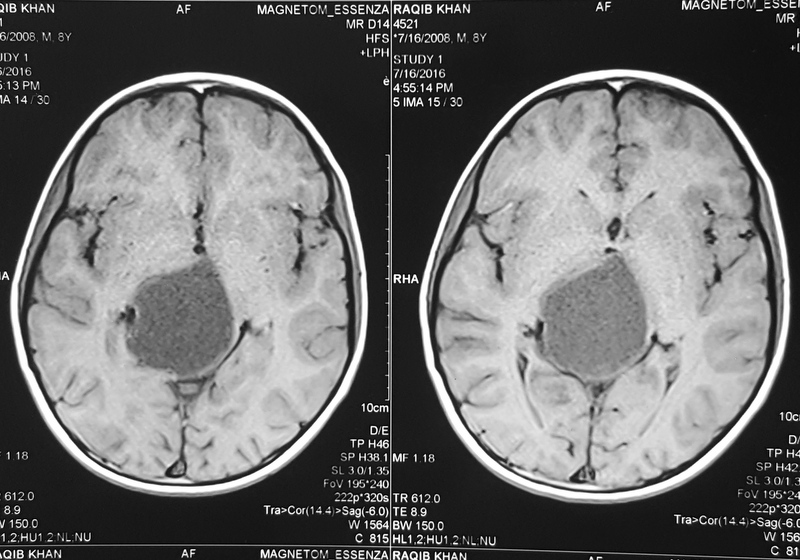
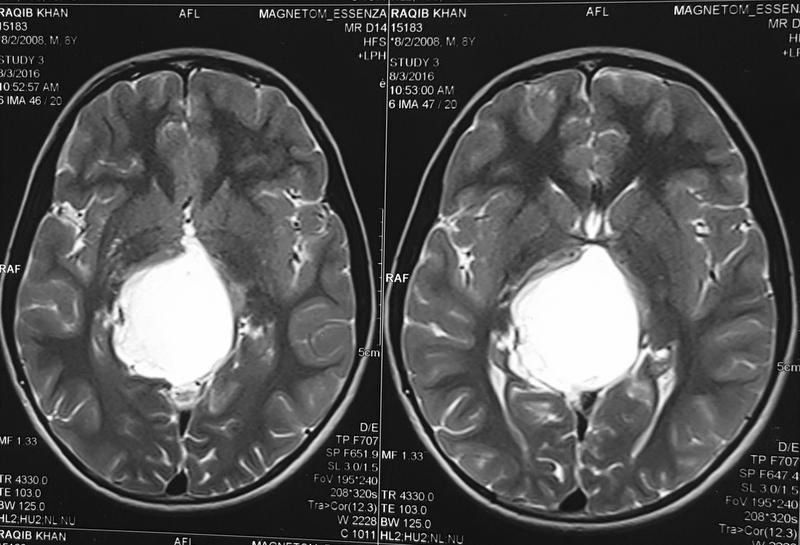
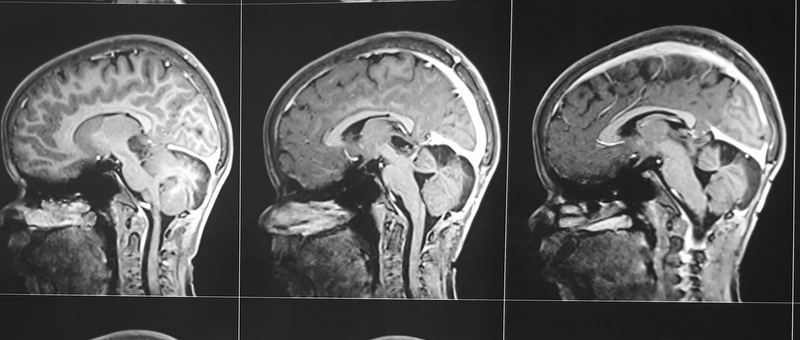
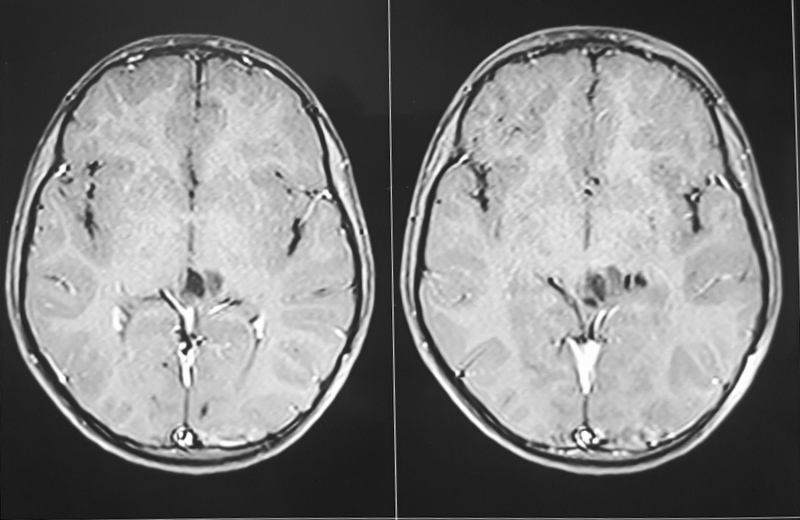
Pilocytic astrocytoma of Posterior Third Ventricle
A 9-year-old male child was evaluated for recurring headaches. Clinically, he had papilloedema. Imaging studies (Figs 1 to 3a & b) showed large posterior third ventricular tumor exhibiting peripheral rim contrast enhancement. The tumour was excised under general anaesthesia, in sitting position, by Supracerebellar Infratentorial approach. The tumour could be excised completely. He has been followed up, and MRI after three years showed only postoperative changes and no tumour residue (Figs 4a & b).